
 Français
FrançaisSurgical abortion
Surgical abortion is an abortion procedure in which intrauterine devices are used to terminate a pregnancy.
The surgical abortion techniques following types are distinguished:
- Vacuum aspiration (vacuum aspiration or “mini-abortion”);
- Curettage (“cleaning”).
Vacuum-aspiration (vacuum aspiration or “mini-abortion”)

The so-called “manual vacuum aspiration” (MVA) technology brought the real boom in gynecology. The technique’s essence is that a vacuum is created with a special syringe. The gynecologist chooses (from different diameters plastic tubes a set) a tube of the most suitable size and inserts it into the uterine cavity. The tube is then connected to a syringe from which air is evacuated. A special mechanism is used to sharply evacuate air from the tube, causing the uterus contents to be sucked by the tube into the syringe.
The term “vacuum-aspiration” refers to the contents suctioning (in our case, the uterine cavity contents) using a vacuum. A tube is inserted into the uterine cavity, connected to negative pressure a source, thereby safely removing the uterine contents. The uterus walls are usually not damaged, and only the endometrium’s superficial (functional) layer is removed. This technique dated back to the last century middle and was widely used in hospitals and some outpatient clinics. In those days, special machines were used to create a vacuum, sometimes rather cumbersome and requiring special conditions for its operation.
Because fetal parts are removed from the uterus by a vacuum means, the technique cannot be used beyond pregnancy 8 weeks. Hence the second name “mini-abortion”.
The “mini-abortion” procedure is moderately painful, so a local anaesthetic is used during the procedure. After the procedure, the patient can go home after 1 hour.
Overall the procedure is quite safe. Pus-inflammatory complications are rare, as the negative pressure directs the flow from the uterine cavity to the outside. Under these conditions, the pathogens’ chance’ entering the uterus is negligible. The uterus mucosa is very rarely damaged deeper than the endometrium surface layer. This ensures that the female body recovery after vacuum aspiration is rapid – usually within 7-10 days.
Limitations: only applicable up to 8 weeks of pregnancy; need to be in hospital or outpatient clinic.
Curettage (“cleaning”)
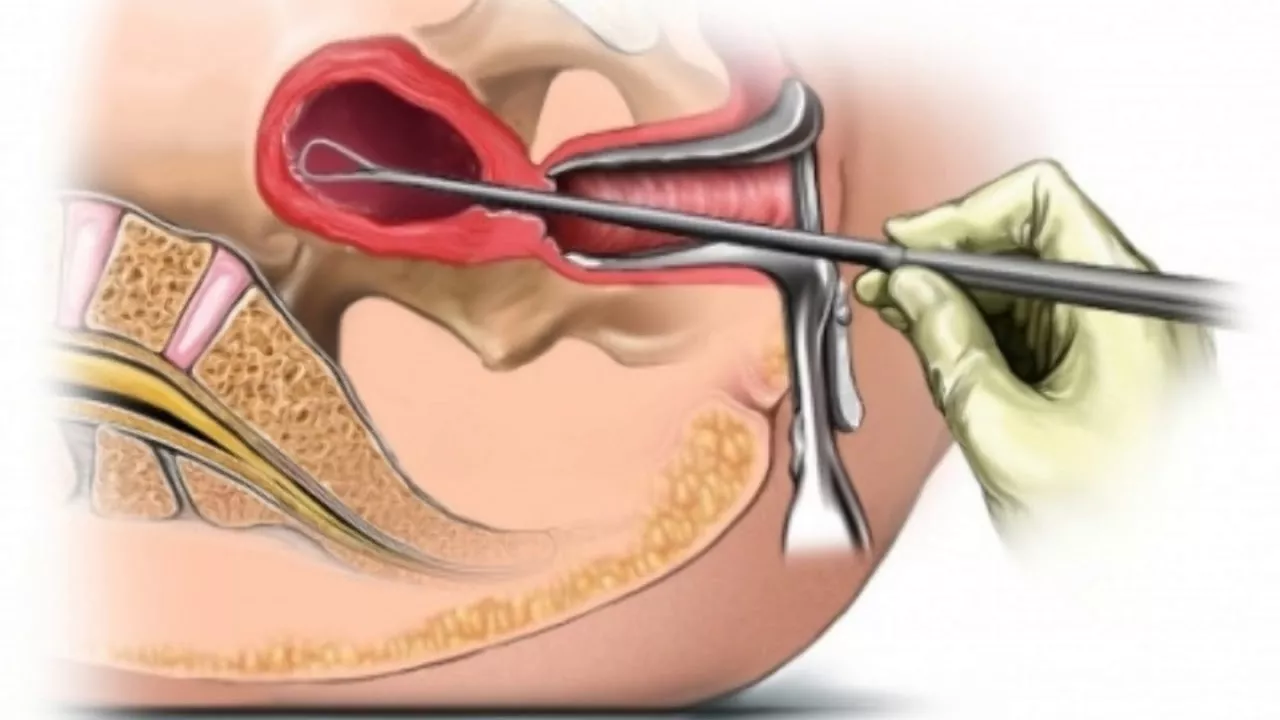
Among gynecologists, this technique is more commonly referred to as “dilatation and curettage, ” which gives the procedure a more accurate description. The method is typically used at higher gestational ages (from 8 to 12 weeks of pregnancy) and is as follows:
- First, the cervical canal is dilated;
- Then the gynaecologist removes the uterus (endometrium) together mucous membrane surface layer with the egg and its membranes with a special instrument (curette). The curette is a thin, long instrument that resembles a noose.
Due to the procedure painful nature, it is carried out under a short-term anaesthetic.
It is the most aggressive method among all abortion techniques, but pregnancy with more than 9 weeks gestational age can only be terminated using the “dilatation and curettage” technique.
The procedure possible complications include:
- Purulent inflammatory processes (endometritis, parametritis, salpingo-oophoritis, pelvic-peritonitis), which can subsequently cause infertility;
- Uterine perforation (or perforation) – although the curette is not a sharp instrument, this complication sometimes occurs.
- Intrauterine synechiae (adhesions) – if the procedure has damaged the endometrium deeper layers on the uterus opposite sides, these “wounds” healing can cause the uterus walls to adhere in these areas.
A woman usually recovers from the procedure within 10-14 days.